What Is the Best Health Insurance for a Family of High Utilizers?
Direction of High-Demand, High-Cost Patients: A Realist and Systematic Review
Research Protocol Dec 4, 2019

I. Groundwork and Objectives for the Review
Background
Payers in the U.S. health intendance organisation, peculiarly Medicare and Medicaid, are increasingly requiring health care systems, coordinated care organizations, and wellness care professionals to progress from payment through fee-for-service arrangements toward alternative payment models that include financial take a chance.1-4 For this reason, the claiming of addressing high-demand, loftier-price (HNHC) patients is increasingly pressing. Health care systems participating in alternative payment models, particularly those that include financial risk, acknowledge that their success in these models depends, in big part, on their effectiveness in addressing the care and costs for HNHC patients.5,six
Although HNHC patients represent a small proportion of the patient population, they account for a substantial proportion of health care costs.7-11 Health care systems would like to attain two goals in relation to HNHC patients: (one) reduce their health care utilise that is potentially preventable or modifiable, which is oftentimes acute intendance in the emergency department (ED) or hospital inpatient setting,12-sixteen and (2) increase their quality of intendance.14-xvi Despite strong motivation to address the burden of HNHC patients, multiple challenges and controversies complicate approaches to identifying HNHC patients and determining the causal mechanisms of complex interventions that affect health care utilization, cost, and quality of care.
Purpose of the Review and Approach
This review has three master objectives, all with the shared purpose of identifying actionable evidence to support informed decisions for clinicians, health care systems, and payers. The first is to draw approaches to identifying HNHC populations. The 2d is to develop and refine theory explaining why particular interventions, in various circumstances, are more likely to be successful in irresolute potentially preventable or modifiable wellness care employ and improving quality of care for HNHC patients. The third is to review the evidence supporting the overall effectiveness of these interventions. We volition use qualitative and quantitative synthesis methods in conducting the review.
Defining High-Need, High-Price Patients
Researchers and practitioners have not decided on a single definition of HNHC patients, those high-need patients for whom high costs are potentially preventable or modifiable. One direct approach is to identify the patients with the highest costs during a historical time menstruation, only no consensus has been reached on the appropriate duration of the time flow and the number and types of utilization.12,13 Likewise, focusing on cost solitary can obscure detecting high-need patients. A large percentage of high-cost patients apply this level of care for a relatively short menstruum of time, and it is the appropriate choice for treating their condition (eastward.one thousand., certain types of cancer or orthopedic surgery patients).17 A 2nd approach is to identify HNHC patients based on diagnoses, such as individuals with multiple co-occurring chronic conditions (i or more of which may be a behavioral health condition).18,19 Relying chiefly on a diagnostic definition, however, ignores that non all high-need patients are HNHC. A large pct of high-need patients use intendance appropriately, even if it may be costly (i.e., needed health care is received through ongoing relationships with primary care and specialist providers). Further refinement in defining and predicting whether individuals with high-demand chronic weather condition are at risk of being high users of potentially preventable or modifiable wellness care may be related to identifying additional hazard factors.xx Overall, HNHC patients include those patients for whom reducing use of high-cost wellness care services in favor of other types of intendance is theorized to result in better care and better outcomes.
To facilitate our synthesis of the evidence on approaches to identifying and describing HNHC patients and to explore the relationships among the approaches, nosotros will carry a "best fit" framework synthesis.21 Consistent with this approach, we begin from an a priori identified framework that we will use to sort show into themes across included studies (i.e., the distinguishing characteristics and reasons why some patients are HNHC). During our review of the evidence, we will use an iterative procedure to consider new themes that are non captured in the initial framework. In the end, nosotros will present a summary of the data and syntheses of the evidence and our conclusions within a framework corresponding to our final conceptual model.
We suggest to begin the synthesis using the taxonomy adult past the National University of Medicine in their report Effective Intendance for High-Need Patients: Opportunities for Improving Outcomes, Value, and Health as our a priori framework.20 This taxonomy groups HNHC patients first based on their clinical and functional characteristics. Amongst the six patient groups presented in the taxonomy, iv run into the inclusion criteria for this review: nonelderly disabled, multiple chronic conditions, major complex chronic condition, and frail elderly. (the additional 2 categories, children with circuitous needs are advancing disease/finish-of-life care are exterior the telescopic of the review.) Inside these assigned groups, the taxonomy proposes boosted, cross-patient grouping assessment based on behavioral health factors and social take chances factors that are believed to influence how individuals use health intendance and increment the chance of receiving fragmented care. Behavioral health factors include persistent and serious mental disease, substance corruption, cognitive decline, and chronic toxic stress. Social risk factors include low socioeconomic status, depression health literacy, social isolation, community impecuniousness, and housing insecurity.
Understanding Interventions for Loftier-Need, High-Cost Patients
To gain a greater understanding of the circuitous culling payment and delivery models, social interventions, and wellness programs that are used to address health care utilization among HNHC patients, we will apply a realist review approach. Consequent with this arroyo, our goal is to explain what works (or fails), for whom, under what circumstances, and why.22 Nosotros will seek to identify, elucidate, and refine the various underlying theories that could explain the arroyo of dissimilar circuitous interventions, explore implementation chains, assess intermediate outcomes, and examine modifications or adaptations applied in various circumstances.22
Using the terminology of the realist approach, reviewers seek to make up one's mind how particular contexts take "triggered" mechanisms to generate outcomes.23 The relationships are summarized equally context + mechanism = result (CMO). Context is the "properties," the variety of features that tin can touch on the implementation of a plan, including participant characteristics, programme setting, resource, and history that trigger or alter the processes through which an intervention produces an consequence.24 Mechanisms are the underlying processes that work in specific contexts to generate the outcomes of interest. The intervention is thought of as manipulating or changing the context and so that specific mechanisms can be triggered.24 Finally, the event is the impact or behaviors that ascend from the inter-relationship between mechanisms and contexts.
Using a systematic review approach, ane would describe a group of studies of interventions equally community health workers whose task is to increment the percentage of patients who regularly get to primary care md office visits. Using a realist arroyo, one would seek to describe why the customs health worker intervention might work. For example, when isolated patients living in a large city, who must exist cocky-reliant in getting to their doctors' appointments are provided with 1-on-one assistance from a community wellness worker on how to employ the bus system (C), the patients are more than probable to get to their role visits (O) because they are more confident and have greater agency that they will be successful (M). A second CMO configuration in the causal pathway might be that regular visits with a clinician (C) issue in greater medication adherence and fewer visits to the ER (O) considering patients trust that their clinicians know them and care nearly their welfare (M).
In addition, to further back up the goal of producing actionable information, we volition also use traditional Evidence-based Do Center systematic review methods to synthesize the prove of the overall effectiveness of the interventions that are included every bit the final focus of the realist portion of the review.
Initial Rough Theory: Controversies and Challenges Regarding Interventions
A realist review begins with an "initial rough theory," a beginning theory of what interventions are expected to exercise. Using this approach, the telescopic, focus, and refinement of the review evolve every bit the review gain; the process includes regular input from stakeholders.24 For this review, nosotros begin broadly, presenting the controversies and challenges in determining the reasons why various interventions or item features of interventions may exist effective in changing HNHC patient health care use.
Describing and Understanding Effective Interventions
In developing the protocol, we conferred with a Cardinal Informant (KI) stakeholder panel to help ensure that the focus of the review would exist relevant to potential cease users. The KI panel consisted of two clinician wellness researchers, one representative of a nongovernmental health policy organization and i representative from a health system research organization; one health organization quality officer; and 1 statistician/survey scientist. (Section IX describes the function of KIs.) KIs differed in their views about the nature of effective interventions for HNHC patients. Some thought that constructive interventions could have broad applicability and be relevant across multiple causes of high utilization. Others thought that constructive interventions need to be targeted to subpopulations of patients; what is effective for ane subpopulation may not exist constructive for another or only effective in certain circumstances and settings. The post-obit are models of organizing the commitment of health care that are theorized as the context for influencing and improving both care commitment and costs for HNHC patients.
Payer-Level Interventions
Accountable Intendance Organizations (ACOs). ACOs align fiscal incentives for intendance coordination and joint financial and health outcome accountability among a large group of wellness care providers across the health care continuum (ambulatory outpatient, acute intendance, postal service-acute care, and home health settings). An supposition underlying success in an ACO model is that providers, whether consciously or unconsciously, act to maximize the health of the patient while as well maximizing their ain financial incentive in caring for the patient. ACOs utilize a multifariousness of strategies to accomplish such goals, including the following:
- Increasing physicians' access to a uniform source of consummate data about patients' health utilization and health condition to support care coordination.
- Using techniques such equally population sectionalisation and risk stratification to focus resources on HNHC populations.
- Using diverse approaches to increasing coordination among health care settings, particularly during transitions between settings in episodes of care:
- outpatient → ED → outpatient
- outpatient → inpatient → mail service-astute care → dwelling house health→ outpatient
Also, increasingly, ACOs include strategies to address social determinants of health. These strategies support the notion that addressing barriers to accessing appropriate health care services is as important every bit coordinating care and ensuring equal access to care.
Patient-Centered Medical Homes (PCMH). The PCMH model encompasses five core attributes: comprehensive care, patient-centered care, coordinated intendance, attainable services, and quality/safety. Although this model is intended to promote changes in price, access, and quality for all patients, it may have the greatest touch on on HNHC patients because HNHC patients can yield the greatest reduction in expenditures and improvement in wellness outcomes. Care coordination is a primal component, particularly during wellness intendance setting transitions (as described above in relation to ACOs), based on the assumption that PCMHs can reduce unnecessary duplication of services and lower preventable utilization of health intendance in plush settings (predominately ED and inpatient care).
The implementation of PCMH models is broadly variable, but most PCMHs encompass the five cadre attributes. The interaction of these five attributes may trigger the mechanisms that produce beneficial impact on health care expenditures and health outcomes of the HNHC population.
Home-Based Primary Care. Home-based principal care moves the commitment of the majority of main intendance from an convalescent function-based setting to a patient's place of residence.25 Intended to be a comprehensive intendance delivery model, this model typically involves a team-based approach and combines home-based care for medical needs with intensive direction and care coordination. Abode-based programs typically serve a population that has a high probability of being HNHC because participants commonly take complex chronic conditions and functional limitations. Home-based master care may benefit HNHC patients if such approaches can better address patients' specific needs, values, and preferences. If HNHC patients have difficulty accessing traditional office-based care, home-based primary intendance may be specially beneficial.
Clinicians are believed to be able to obtain greater insight into patient needs with habitation visits, often finding ecology and nonmedical factors related to patients' problems. HNHC patients may require frequent monitoring, intense direction, or rapid follow-up that cannot be easily accommodated past an office-based provider. Home-based primary care may also be able to help HNHC patients avoid complications from hospital care (e.g., certain infections, delirium) when hospitalizations themselves can exist averted or shortened. Several additional assumptions underlying the success of this approach is that the HNHC patients can be identified, that intervening at domicile is price-effective, and that the teams work well together.
Health System and Provider-Level Interventions
At the health system and clinician levels, data tin can be used to report wellness care service utilize that may signal that a patient is HNHC and needs additional services. ED alerts inform clinicians that a patient has received care in the ED, which can assistance them identify patients whose patterns of care might be considered HNHC and in need of additional support services. Hotspotting uses data to place patients whose costs are outliers, such as the HNHC population; empathize the trouble; dedicate resources; and design effective interventions.26 Hotspotting typically includes multidisciplinary, coordinated care that treats the whole patient and attends to the nonmedical and social determinants that affect wellness, including housing, mental health, substance abuse, and emotional support. The underlying premise is that intensive and highly individualized care, addressing the unique needs of an HNHC patient, including social determinants of wellness, will improve health outcomes and reduce health expenditures beyond the toll of the high intensity, highly individualized hotspotting intervention.
Health-Related Interventions
At the patient level, supportive services and social determinants of wellness-related interventions tin can bear on the success or failure of circuitous social interventions. They are intended to span the gap betwixt health care professionals who evangelize direct care and an individual patient. Persons in a multifariousness of roles may provide supportive services, such as social workers, community wellness workers, patient navigators, and peer-to-peer networks.
Patient support services are intended to accost mutual barriers related to resource limitations, education, and treatment adherence, thereby improving patient outcomes. Relatedly, the surroundings and social determinants of health, such equally low income, poor teaching and diet, homelessness, and lack of transportation, accept been identified as predisposing factors limiting access to care. For example, stable housing could better patients' ability to interact consistently with their wellness intendance providers and social support systems, which, in turn, could increase adherence to their treatment program.27
Applying a Articulate Classification Taxonomy
A challenge in conducting a review on direction of HNHC patients is the absence of a consensus in the field of a unifying classification schema or taxonomy of interventions. This gap complicates organizing key dimensions of these interventions into meaningful distinctions for group and separating their components.28
Intervention nomenclature in recent systematic reviews regarding HNHC patients differs significantly. One systematic review stratified interventions as domicile-based, dispensary-based, and primary intendance augmentation.15 Another categorized interventions into case direction, private care plans, and data sharing.thirteen Baker and colleagues stratified interventions past population type: adults (i) with ii or more chronic diseases, (ii) with one chronic disease and depression, and (3) identified as at adventure for high health care utilization.14
We suggest to organize our findings starting with a taxonomy of interventions that maps to mechanisms that the review team theorizes are related to the success of interventions for HNHC patients. We will attempt to separately address context, outcomes, and mechanisms at the payer, health care arrangement, provider, and patient levels and those that cut across interventions.
II. The Key Questions
Key Questions Initially proposed Key Questions (KQs) were posted for public comment Feb 7, 2019, through March 7, 2019. Nosotros received comments from two individuals. The kickoff private wrote, "Equally of import as identifying high utilization/high cost patients is understanding patterns of persistence from yr to year. That is critical for prioritization of interventions and the most effective interventions for patients with i or two years of high cost versus multiple ongoing years." Nosotros agree with the comment. In describing HNHC patients (KQ 1), we will limit the population to individuals with at to the lowest degree 1 twelvemonth of high-price intendance. Within that population, nosotros volition present the patterns of persistent wellness care use and costs described in the studies. The second private commented that existence breastfed is a "stiff heath indicator" and would like the review to include the relationship between having been breastfed equally a kid and being HNHC every bit an developed. While this may be a salient characteristic of the HNHC population, for this assay, nosotros need to exist able to discover past or predicted high utilization. We did not observe whatsoever studies that examine the relationship between breastfeeding in infancy with loftier utilization in adulthood.
Table i outlines the noun changes betwixt the preliminary KQs and those included in this protocol. The "final" KQs appear below the table.
Table one. Changes to KQs and PICOTS
| Original Element | Source | Comment | Conclusion and Changes | Rationale (Implications for Show Written report) |
|---|---|---|---|---|
| Population name | KI | KIs thought the term "high utilizer" should be changed to "loftier- need, high-toll (HNHC)," which has become a more commonly used term. | Modify made | No implications for the workload of the review |
| KQ 1 | EPC | The EPC modified KQ 1. KQ 1a-KQ 1e accept not been modified. | Original question: What are the characteristics of patients who are "high utilizers"? Protocol revised question: (see beneath) | The EPC modified KQ 1 for clarity. |
| KQ 2 | EPC | The EPC modified KQ ii to follow the format of a realist review. | Original question: What are the effective interventions for adults identified as loftier utilizers of wellness care? Protocol revised question: (see below) | The EPC modified KQ two to answer this question using a realist review arroyo. The edits are intended to support the goal of understanding the mechanisms that explicate successful outcomes in complex interventions serving HNHC patients. |
| KQ iii | EPC | The EPC intends to respond KQ 3, using systematic review methods to back up the findings apropos the interventions included in answering KQ two, using realist review methods. | Original question: Overall, what is the evidence most which interventions targeting which patient groups lead to the highest overall improvement in health outcomes and cost savings for patients, clinicians, providers, and payers? Protocol revised question: (run into beneath) | The original question was a comparative effectiveness question. Based on our conversations with KIs and our initial review of the literature, we believe that it will exist valuable to the field to focus on the more key question of why and how particular interventions work (KQ 2) and the evidence of effectiveness and harms of these interventions (KQ 3). |
EPC = Evidence-based Exercise Center; HNHC = loftier-need, high-cost; KI = Key Informant; KQ = Key Question.
- KQ 1 ("best fit" framework synthesis): What criteria identify or tin be used to predict that patients will be HNHC and why?
- KQ 1a. How do criteria comprise patient clinical characteristics?
- KQ 1b. How do criteria incorporate patient health behaviors and sociodemographic characteristics (east.g., age, social determinants of wellness, insurance condition and source of coverage, and access to the wellness intendance system)?
- KQ 1c. How do criteria incorporate types, amount, duration, and patterns of persistent use of potentially preventable or modifiable health care employ?
- KQ 1d. Do criteria differ at the payer, wellness care system, or provider levels?
- KQ 1e. How tin can observed or predicted potentially preventable or modifiable high use of health care be differentiated from necessary and advisable use?
- KQ two (realist review): What are the mechanisms that pb to reductions in potentially preventable or modifiable health care utilize and result in improved health outcomes and cost savings in interventions serving HNHC patients?
- KQ 2a. What are the of import contexts, such as the characteristics of the HNHC patients, the broader health care delivery system, and the community, that impact whether mechanisms facilitate the desired outcomes?
- KQ 3 (systematic review): Overall, what is the effectiveness and harms of interventions, included in answering KQ two, in reducing potentially preventable or modifiable wellness care use and costs and improving wellness outcomes among HNHC patients?
PICOTS and Nomenclature Taxonomy
Nosotros fabricated no substantive changes to the population, interventions, comparators, outcomes, timing, settings, and study design (PICOTS). As we go along with the review, nosotros conceptualize that we will further focus our analysis and desire to discuss decisions with our Technical Expert Panel (TEP) on multiple occasions. These occasions tin can include any or all of the following:
- Receiving input on whether nosotros have identified the relevant studies or programs and, if we have not, where to discover additional information.
- Refining the HNHC population for the purposes of the review, including whether to combine subpopulations or keep them carve up.
- Discussing the theories of why and when various mechanisms are activated past effective complex interventions inside particular contexts to produce outcomes.
Our final goal is to present our findings within the context of a unifying nomenclature schema or taxonomy. We may seek feedback from our TEP and members of our KI stakeholder panel on whether what we develop will be useful to individuals and organizations that are seeking actionable data.
Three. Analytic Framework
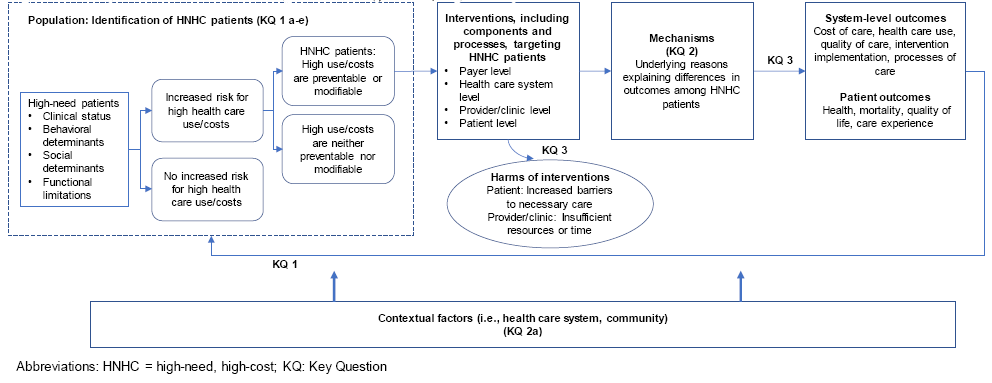
Figure 1 presents the analytic framework for the review and depicts the KQs in relation to the PICOTS. The effigy illustrates how HNHC patients may be identified, how interventions that target HNHC patients together with contextual factors trigger dissimilar mechanisms of action that may effect in systems-level outcomes (i.e., cost, utilization, and quality of care) and patient outcomes (i.e., wellness, mortality, and patient experience), and harms that may occur considering of the interventions.
Figure 1. Analytic framework for management of high-need, loftier-cost patients
IV. Methods
Criteria for Inclusion/Exclusion of Studies in the Review
Table 2 presents the initial inclusion and exclusion criteria for the PICOTS of the review. In keeping with realist review methods, we will refine the telescopic of the review as we uncover evidence and focus the depth and latitude of the review.29 We will accost KQ ane using a "all-time fit" framework synthesis methodology and KQ 2 using a realist review methodology; with these approaches, all study designs, if relevant, are admissible for inclusion. We will answer KQ 3 using a systematic review methodology, resulting in open-door written report designs being more than limited.
Table 2. Inclusion/exclusion table
| PICOTS | Inclusion | Exclusion |
|---|---|---|
| Population | KQs i, 2, and 3: Noninstitutionalized adults, eighteen years of age or older. KQ 1: One or more years of potentially preventable or modifiable high health care toll and/or use. KQs 2 and 3, two groups: | Patients receiving a high level of health intendance services that are considered appropriate for their status OR high level of health intendance services are measured for less than i year OR terminate-of-life care |
| Intervention | KQ 1: Not relevant, interventions not necessary for inclusion. KQs two and 3: | KQs 2 and three: Interventions for which the relevance for and impact on HNHC patients cannot exist determined. |
| Comparator | KQ 1: Comparison population or no comparator KQ 2: Any intervention, treatment as usual, or no comparator intervention. | KQ 3: No comparator |
| Outcomes | KQ 1: Population characteristics described or predicted. KQs i, ii, and three: | All other outcomes, including behavioral health outcomes |
| Time frame | Potentially preventable or modifiable loftier cost wellness intendance use measured for one year or more. KQ 3: Measurement of outcomes at i twelvemonth or more than afterward implementation of the intervention. | Shorter time periods |
| Settings | Health care and support services delivery settings, including outpatient, ED, the broader wellness care delivery environs, community characteristics related to social determinants of wellness. KQ 1: United States. KQs two and three: patient-level interventions: very loftier human being development index countries; Wellness arrangement or payer-level interventions: United States. | Institutional care settings, such every bit hospitals, skilled nursing, long-term care facilities, and prisons or jails |
| Study design | KQs 1 and 2: All study designs except reviews summarizing across original studies or interventions. KQ three: Randomized controlled trials, cluster randomized trials, cohort studies, case-control studies, quasi-experimental designs with a comparison group. | KQ 3: All other designs |
| Language | Studies published in English | Studies published in languages other than English |
| Publication Type | All publications that allow abstraction and estimation of findings | KQ 3 just: Abstract-only publications |
ACO = Accountable Care Organization; ED = emergency department; EMS = emergency management services; HNHC = high-need loftier-toll; KQ = Key Question; PICOTS = population, intervention, comparator, outcomes, time frame, settings
Searching for the Testify: Literature Search Strategies to Place Relevant Studies to Answer the Cardinal Questions
Areas of Focus for Searches
Nosotros will behave this review post-obit the methodology of a "best fit" framework synthesis (for KQ 1), realist review (for KQ 2), and a systematic review (for KQ 3).22 In conducting the realist review, nosotros conceptualize that starting from our rough theory, our searches will be iterative in a way that will enable the states to uncover the underlying mechanisms in complex interventions that are related to approaches or components that may be constructive with HNHC patients in different contexts and why.
To answer KQ ane, our goal is to review the evidence to develop an actionable clarification of HNHC patients that captures the distinguishing characteristics of populations whose high utilization is potentially modifiable. Based on input from our KI stakeholders during evolution of the protocol, HNHC populations will be identified in our searches through unlike approaches, including the following:
- Multiple health conditions (i.e., multiple co-occurring chronic weather, including behavioral health conditions).
- Multiple health weather coupled with additional risk factors (i.due east., functional limitations, behavioral factors, financial factors, or social risk factors).
- Health services use (due east.chiliad., overuse of ED, inpatient, or other high-toll services).
To answer KQs 2 and 3, our attention will focus on the following kinds of interventions:
- Complex structural changes and alternative financial arrangements (due east.chiliad., ACOs, PCMHs, and wellness homes).
- Novel approaches to delivering services and providing information to clinicians (e.g., interdisciplinary teams, hotspotting).
- Calculation any patient-centered component to an existing wellness intendance commitment arrangement (e.chiliad., patient navigator, peer support, and caregiver supports).
Nosotros as well expect relevant interventions to be a source for further defining populations of interest.
Sources of Literature
To begin to identify articles relevant to the review, nosotros initially conducted a focused search of MEDLINE via PubMed search (Appendix A). Our broader search will include both databases and gray literature sites, including Cochrane Clinical Trials Central Register, PsycINFO, Cumulative Index of Nursing and Allied Health Literature, EMBASE, Web of Science, Clinicaltrials.gov, and Academic Search Premier.
Our overall search results fall into iii "buckets" because we will need to use more than than one approach to finding the literature that identifies HNHC patient populations and, relatedly, relevant interventions. The buckets are as follows:
- Studies identifying the population by using the text terms "high utilizer/medically complex/high needs" and similar terms. Medical Subject field Heading (MeSH) terms are not bachelor to identify the population using these types of terms.
- Studies identifying the population by using the MeSH term "multiple chronic weather condition" or like terms, limited to individuals with functional limitations, behavioral factors (e.k., health take a chance behaviors or serious mental illness), or social risk factors.
- Studies identifying populations past limiting them to specific weather condition or combinations of weather condition (e.yard., cardiovascular disease, diabetes, or both), when such populations likewise had functional limitations or behavioral or social take a chance factors.
We will also search for evaluation reports or other gray literature on regime websites. These will include the following: the Centers for Medicare & Medicaid Services, specially its Center for Medicare and Medicaid Innovation, which supports development of Medicaid demonstrations and other culling payment models; the National Institute on Drug Abuse; the Centers for Disease Control and Prevention; the National Establish on Aging; the Human Resources Services Administration; the Veterans Administration; the National Library of Medicine (for HSRProj), and Social Work Abstracts. Nongovernment-sponsored studies volition be searched on websites of such organizations as the Camden Coalition, the Center for Health Intendance Strategies, the Commonwealth Fund, the Kaiser Family unit Foundation, the Milbank Memorial Fund, the National Academy of Medicine, Patient-Centered Outcomes Research Institute, the Robert Woods Johnson Foundation, and the Social Interventions Research & Evaluation Network Prove Library.
Following our preliminary searches as recommended for a realist review, we volition bear snowball searches, including reviewing reference lists of included studies, identifying whether included studies are cited in newer articles, and looking for related studies, such every bit those suggested by PubMed.thirty In addition, we know that we will need to relax our population restrictions to examine whether some studies of interventions, such every bit those related to ACOs, health homes, community health workers, patient navigators, care managers, and others, focus on patients who are at risk of existence HNHC and thus may non be identified through one of our 3 population buckets.
Quality Balls for Searches
We volition bear quality checks to ensure our search identifies known studies. If not, we will revise and rerun our searches. An experienced librarian familiar with systematic reviews volition design and carry all searches in consultation with the review team. We will likewise acquit an updated literature search (of the same databases searched initially) concurrent with the process for peer and public review of the typhoon study. We will investigate any literature that peer reviewers or the public suggest and, if appropriate, volition contain them into the final review. We will identify all eligible studies using the same criteria described above.
Data Abstraction and Data Management
As with systematic reviews, a wide range of documents tin exist relevant in a realist synthesis. Two trained research team members volition independently review all titles and abstracts identified through searches for eligibility against our inclusion/exclusion criteria using Abstrackr.31 Studies marked for possible inclusion by either reviewer will undergo a full-text review. For studies without adequate information to determine inclusion or exclusion, we volition retrieve the full text and then make the determination. All results volition be tracked in an EndNote® bibliographic database (Thomson Reuters, New York, NY).
Nosotros will think and review the total text of all titles included during the title/abstract review stage and through manus searches. Two trained team members volition independently review each full-text article for inclusion or exclusion based on the eligibility criteria described to a higher place (Tabular array 3). If both reviewers agree that a study does non meet the eligibility criteria, the study will be excluded. If the reviewers disagree, conflicts volition exist resolved by discussion and consensus or by consulting a third fellow member of the review squad. Equally described to a higher place, all results will be tracked in an EndNote database.
For the realist review, we will evaluate articles for their relevance and robustness in answering the review questions and their contribution to theory edifice and testing. For all KQs, nosotros will too evaluate manufactures as to whether the methods that authors used to generate data are apparent and trustworthy.29 We will record the reason that we concluded that any excluded total text did not satisfy the eligibility criteria so that nosotros can afterwards compile a comprehensive list of such studies.
For studies that run across our inclusion criteria, we will abstruse relevant information into tables. To answer the realist review question (KQ ii), we volition abstract data relevant for our analyses and synthesis, including context, intervention, mechanisms, outcomes, and theories. Nosotros await to refine the data extraction process continually as the review progresses; we anticipate data choice and appraisement will be ongoing and conducted in parallel with the assay.29
To answer the systematic review question (KQ 3), nosotros will design show tables to gather pertinent information from each article; these information will include characteristics of study populations, settings, interventions, comparators, study designs, methods, and results. Trained reviewers will extract the relevant data from each included commodity into the evidence tables. A second fellow member of the team volition review all data abstractions for completeness and accuracy.
Realist Review: Quality Appraisal
Quality appraisal in realistic reviews is not focused on assessing the risk of bias of individual studies merely rather on assessing the rigor used to develop one or more programme theories. In realist reviews, assessing study rigor occurs throughout the process of synthesis and includes all of the key aspects of the review procedure: the quality of the theory development, the data identified as relevant and analyzed, and the inferences fabricated from the data.32
Nosotros volition, therefore, appraise data based on relevance (whether included articles can contribute to theory edifice and testing), trustworthiness (whether the data in a written report have been obtained empirically, using methods that are conspicuously stated and whether the data could exist found in more than one source), plausibility of the argument underlying the theory (the coherence of the argument, including its breadth in explaining the data, its simplicity and fit with existing theory), and rigor (whether included articles are methodologically credible with regard to outcomes reported and methods used for testing propositions). Our appraisal approach will consider how our findings (theory and observation of relationships) have evolved at each evidential step. Every bit such, we will use RAMESES project standards to guide our judgments in quality appraisal tasks.29,32-34
Previous realist reviews take practical qualitative methods to appraisement. Standards tools include the UK Cabinet Office quality framework and a Critical Appraisal Skills Programme tool.34 Withal, according to a study comparison appraisement methods in realist reviews, Dixon-Wood et al.35 found tool-based approaches to be like in the level of agreement to those using unprompted judgment.
Assessment of Methodological Quality or Risk of Bias of Individual Studies
For KQs 1 and 2, nosotros will appraise each included qualitative enquiry study in terms of rigor and validity using the Critical Appraisement Skills Plan checklist for qualitative enquiry.38 Our goal is to have a consistent approach for evaluating the strengths and limitations in private studies. Still, equally recommended by the authors of the checklist, the results will not exist used to create a scoring system. Descriptive studies that count or seek to place characteristics of HNHC patients will be assessed in relation to the threat of selection bias and confounding, equally relevant. Other studies, such as theory and opinion used to answer KQ 2, will be solely appraised using the realist review quality appraisal approach discussed above.
For KQ 3, we will use the criteria set forth past the Agency for Healthcare Quality and Research'south (AHRQ'southward) Methods Guide for Comparative Effectiveness Reviews. To assess the take chances of bias (i.e., internal validity), nosotros will apply the ROBINS-139 tool for observational studies and the Cochrane randomized controlled trial (RCT) tool40 for RCTs. For both RCTs and observational studies, adventure of bias assessment will include questions to assess all the post-obit:
- Diverse types of bias, including choice bias, confounding, operation bias, detection bias, and attrition bias.
- Concepts near adequacy of randomization (for RCTs merely), such as similarity of groups at baseline, and masking.
- Method of handling dropouts and missing information, whether intention-to-treat assay was used, reliability and validity of result measures, and handling fidelity.41
Ii contained reviewers will assign chance of bias ratings for outcomes from each report; they will too specify when the risk of bias for an individual outcome may be lower than the rating for the report overall. Disagreements between the ii reviewers will be resolved by give-and-take and consensus or by consulting a 3rd member of the team.
We volition give a low run a risk of bias rating for outcomes that meet all criteria. Studies that do not written report their methods sufficiently may be rated every bit unclear risk of bias. We will give a high take a chance of bias rating to outcomes from studies that have a methodological shortcoming in i or more categories and will exclude them from our main analyses.
Information Synthesis
Realist Review: Three Master Targets of Analysis
In a realist review, the goal of the synthesis is to develop so "exam" (confirm, refute, or refine), against the data from included documents, realist causal explanations for outcomes. Analysis of the data should likewise be directed to agreement the relationships of the CMO configurations that have been developed within the program theory or theories. The realist causal caption for outcomes takes the form of CMO configurations. Specifically, a CMO configuration describes and explains the relationship between particular features that take been interpreted as functioning as context, particular mechanisms, and particular outcomes. In a sentence, such a CMO presentation volition take the form of "In 'X' context, 'Y' mechanism is activated or triggered, and it causes 'Z' outcome." The synthesis presents evidence to back up two master conclusions: (1) that the specific features of context exist and bear on the activation of a machinery of activeness (entities, processes, or structures) and (2) that the hypothesized mechanisms exist and cause outcomes.24
Systematic Review: Procedures for Analysis and Synthesis
For KQ 3, we will follow standard EPC (AHRQ) procedures to summarize all included studies in narrative course and in summary tables that tabulate the important features of the written report populations, blueprint, intervention, outcomes, setting (including geographic location), and results. Autonomously from documenting basic study characteristics, we will include findings only from studies of low, medium, or unclear chance of bias in our main report, which we will synthesize either qualitatively or quantitatively (insofar as possible).
Findings from studies determined to be of high risk of bias will announced in the testify tables in the appendix. If feasible, we may do qualitative or quantitative sensitivity analyses to gauge the difference in conclusions stemming from including and excluding studies considered loftier risk of bias.
If nosotros detect three or more than studies for a comparison of an outcome of interest, we volition consider pooling our findings by using quantitative assay (i.e., meta-assay) of the data from those studies. Nosotros will besides consider conducting network meta-analysis using Bayesian methods to compare the interventions with each other if we identify at least three studies that tested the same intervention with a common comparator. For all analyses, we will utilize random furnishings models to approximate pooled or comparative furnishings; different a fixed-furnishings model, this approach allows for the likelihood that the truthful population effect may vary from written report to report. To determine whether quantitative analyses are appropriate, we will assess the clinical and methodological heterogeneity of the studies nether consideration post-obit established guidance.
Systematic Review: Grading the Strength of Show
For KQ 3, nosotros will grade the strength of testify (SOE) based on the guidance established for the EPC Program.42 Developed to grade the overall force of a body of show, this approach incorporates five cardinal domains: risk of bias (includes study design and aggregate quality), consistency, directness, precision of the evidence, and reporting bias. It as well considers other optional domains that may be relevant for some scenarios, such as a dose-response association, plausible confounding that would decrease the observed result, and force of clan (magnitude of effect).
Table 3 describes the grades of evidence that can be assigned. Grades reflect the force of the body of bear witness to answer KQs on the effectiveness and harms of the interventions included in this review. Ii reviewers volition assess each domain for each cardinal outcome; they will resolve whatsoever differences by consensus give-and-take. If the volume of evidence is large, nosotros may focus the SOE grading on outcomes of substantial importance to decisionmakers and those unremarkably reported in the literature.
Table 3. Definitions of the grades of overall strength of evidence42
| Grade | Definition |
|---|---|
| High | High confidence that the show reflects the truthful event. Further research is very unlikely to change our confidence in the guess of consequence. |
| Moderate | Moderate confidence that the bear witness reflects the true event. Further research may change our confidence in the guess of the effect and may change the estimate. |
| Low | Depression conviction that the evidence reflects the truthful result. Farther research is likely to change our confidence in the gauge of the issue and is likely to alter the approximate. |
| Insufficient | Evidence either is unavailable or does not permit interpretation of an upshot. |
Assessing Applicability
We will assess the applicability of individual studies as well as the applicability of a trunk of testify following guidance from the Methods Guide for Effectiveness and Comparative Effectiveness Reviews.43 We look to be able to practise this for all three KQs.
For private studies, we volition examine conditions that may limit applicability based on the PICOTS structure. The cess of applicability is integral to a realist review through its consideration of context within CMO configurations. We will nowadays when patterns across studies either were not tested or practise not appear to operate similarly in detail settings.
5. References
i. Centers for Medicare & Medicaid Services. CMS proposes "pathways to success," an overhaul of Medicare'southward ACO programme. Baltimore, Physician: Centers for Medicare & Medicaid Service; 2018. https://world wide web.cms.gov/newsroom/press-releases/cms-proposes-pathways-success-overhaul-medicares-aco-program?_ga=2.111400452.1093732935.1551231053-96630637.1551231053. Accessed on February 27,, 2018.
two. Centers for Medicare & Medicaid Services. Medicare-Medicaid accountable care organisation (ACO) model. Baltimore, MD: Centers for Medicare & Medicaid Services; 2016. https://www.cms.gov/newsroom/fact-sheets/medicare-medicaid-accountable-care-arrangement-aco-model. Accessed on February 27,, 2019.
3. Centers for Medicare & Medicaid Services. Vermont all-payer ACO model. Baltimore, MD: Centers for Medicare & Medicaid Services; 2016. https://www.cms.gov/newsroom/fact-sheets/vermont-all-payer-aco-model. Accessed on February 27,, 2019.
4. Centers for Medicare & Medicaid Services. CMS finalizes "pathways to success," an overhaul of Medicare's national ACO programme. Baltimore, MD: Centers for Medicare & Medicaid Services; 2018. https://world wide web.cms.gov/newsroom/printing-releases/cms-finalizes-pathways-success-overhaul-medicares-national-aco-program. Accessed on February 27,, 2019.
five. Brennan A, Gaus C. ACOs at a crossroads: costs, chance and MACRA. A NAACOS policy white paper. Washington, DC: National Association of ACOs,; 2016. https://www.naacos.com/acos-at-a-crossroads Accessed on Feb 27,, 2019.
6. Hagland M. NAACOS and ACO leaders express distress over just-appear MSSP application deadline. Sarasota, FL: Healthcare Innovation; 2019. https://www.hcinnovationgroup.com/population-health-management/article/13031036/naacos-and-aco-leaders-express-distress-over-justannounced-mssp-application-deadline. Accessed on February 27,, 2019.
7. Cohen Due south. The concentration of health care expenditures and related expenses for costly medical conditions, 2012. Statistical Brief #455. Rockville, Dr.: Agency for Healthcare Inquiry and Quality; 2014. http://world wide web.meps.ahrq.gov/mepsweb/data_files/publications/st455/stat455.pdf.
viii. Cohen SB. The concentration and persistence in the level of health expenditures over time: estimates for the U.South. population, 2011–2012. Statistical Brief #449. Rockville, Doctor: Bureau for Healthcare Research and Quality; September 2014. http://world wide web.meps.ahrq.gov/mepsweb/data_files/publications/st449/stat449.shtml.
ix. Cohen SB. The concentration of health intendance expenditures in the U.S. and predictions of future spending. J Econ Soc Meas. 2016;41:167–89.
x. Centers for Medicare & Medicaid Services. Medicare beneficiaries at a glance. Baltimore, Medico: Centers for Medicare & Medicaid Services; 2019. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Casher-Snapshot/Bene_Snapshot.html. Accessed on Feb 27,, 2019.
eleven. Centers for Medicare & Medicaid Services. All Medicare inpatient hospitals: utilization, program payments, and toll sharing for original medicare beneficiaries, past demographic characteristics and Medicare-Medicaid enrollment condition, calendar year 2017. Baltimore, MD: Centers for Medicare & Medicaid Services; n.d. https://www.cms.gov/Inquiry-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/CMSProgramStatistics/2017/Downloads/UTIL/2017_CPS_MDCR_INPT_HOSP_2.PDF. Accessed on February 27,, 2019.
12. Moe J, Kirkland SW, Rawe East, et al. Effectiveness of interventions to subtract emergency department visits by adult frequent users: a systematic review. Acad Emerg Med. 2017 Jan;24(1):40-52. doi: 10.1111/acem.13060. PMID: 27473387.
13. Soril LJ, Leggett LE, Lorenzetti DL, et al. Reducing frequent visits to the emergency section: a systematic review of interventions. PLoS One. 2015;ten(4):e0123660. doi: 10.1371/periodical.pone.0123660. PMID: 25874866.
xiv. Baker JM, Grant RW, Gopalan A. A systematic review of care management interventions targeting multimorbidity and high care utilization. BMC Health Serv Res. 2018 Jan 30;18(1):65. doi: ten.1186/s12913-018-2881-8. PMID: 29382327.
15. Edwards ST, Peterson K, Chan B, et al. Effectiveness of intensive main care interventions: a systematic review. J Gen Intern Med. 2017 Dec;32(12):1377-86. doi: ten.1007/s11606-017-4174-z. PMID: 28924747.
xvi. Smith SM, Wallace Eastward, O'Dowd T, et al. Interventions for improving outcomes in patients with multimorbidity in chief intendance and community settings. Cochrane Database Syst Rev. 2016 Mar 14;3:CD006560. doi: 10.1002/14651858.CD006560.pub3. PMID: 26976529.
17. Cohen S, Yu West. The concentration and persistence in the level of health expenditures over time: estimates for the U.Due south. population, 2008–2009. Statistical Cursory #354. Rockville, Md: Agency for Healthcare Research and Quality; January 2012. http://www.meps.ahrq.gov/mepsweb/data_files/publications/st354/stat354.pdf.
18. Pearson SD, Katzelnick DJ, Simon GE, et al. Depression among high utilizers of medical care. J Gen Intern Med. 1999;fourteen(viii):461-eight. doi: 10.1046/j.1525-1497.1999.06278.x.
19. Katon W, Von Korff M, Lin E, et al. Distressed loftier utilizers of medical care. DSM-III-R diagnoses and handling needs. Gen Hosp Psychiatry. 1990;12(6):355‐62. PMID: CN-00071507.
20. National Academy of Medicine. Effective care for high-need patients. Opportunities for improving outcomes, value, and health. Washington, DC: National Academy of Sciences; 2017.
21. Carroll C, Booth A, Leaviss J, et al. "Best fit" framework synthesis: refining the method. BMC Med Res Methodol. 2013 Mar 13;13:37. doi: 10.1186/1471-2288-xiii-37. PMID: 23497061.
22. Pawson R, Greenhalgh T, Harvey G, et al. Realist review--a new method of systematic review designed for complex policy interventions. J Health Serv Res Policy. 2005 Jul;x(Suppl 1):21-34. doi: 10.1258/1355819054308530. PMID: 16053581.
23. Greenhalgh T, Wong G, Westhorp G, et al. Protocol--realist and meta-narrative evidence synthesis: evolving standards (RAMESES). BMC Med Res Methodol. 2011;xi:115-. doi: 10.1186/1471-2288-11-115. PMID: 21843376.
24. Wong K, Westhorp G, Pawson R, et al. Realist synthesis RAMESES training materials London: National Institute for Wellness Enquiry Health Services and Delivery Research Programme; July 2013.
25. Totten A, White-Chu E, Wasson N, et al. Home-based chief care interventions. Comparative Effectiveness Review No. 164. (Prepared by the Pacific Northwest Prove-based Practice Eye under Contract No. 290-2012-00014-I.). AHRQ Publication No. xv(xvi)-EHC036-EF. Rockville, MD: Agency for Healthcare Research and Quality; February 2016.
26. Clan of American Medical Colleges. Hot spotting guide FAQ. Washington, DC: Association of American Medical Colleges; 2019. https://www.aamc.org/initiatives/hotspotter/faqs/372468/hotspottingguidefaq.html. Accessed on Baronial 12, 2019.
27. National Association of Community Health Centers. Health intendance for the homeless. Bethesda, Md: National Association of Community Health Centers, Inc.; 2019. http://www.nachc.org/wellness-center-issues/special-populations/health-care-for-the-homeless/. Accessed on August 12, 2019.
28. Guise JM, Chang C, Butler Chiliad, et al. AHRQ serial on complex intervention systematic reviews-paper 1: an introduction to a series of articles that provide guidance and tools for reviews of complex interventions. J Clin Epidemiol. 2017 Oct;90:6-x. doi: 10.1016/j.jclinepi.2017.06.011. PMID: 28720511.
29. RAMESES Project. Quality standards for realist synthesis (for researchers and peer-reviewers). Oxford: Nuffield Department of Master Care Health Sciences, University of Oxford; 2014. world wide web.ramesesproject.org). Accessed on August 12, 2019.
30. Wong G, Greenhalgh T, Westhorp Thou, et al. Development of methodological guidance, publication standards and preparation materials for realist and meta-narrative reviews: the RAMESES (Realist and Meta-narrative Evidence Synthesis - Evolving Standards) project. Health Services and Commitment Enquiry 2014;2 doi: ten.3310/hsdr02300.
31. Wallace BC, Minor Thousand, Brodley CE, et al. Deploying an interactive machine learning arrangement in an bear witness-based practice center: Abstrackr. Proc. of the ACM International Health Computer science Symposium (IHI); 2012. 1038: pp. 819-24.
32. Wong K. Data gathering for realist reviews: Looking for needles in haystacks. In: Emmel N, Greenhalgh J, Manzano A, Monaghan M, Dalkin Southward, eds. Doing realist research. London: Sage; 2018.
33. Wong G, Greenhalgh T, Westhorp Thousand, et al. RAMESES publication standards: realist syntheses. BMC Med. 2013 2013/01/29;xi(1):21. doi: x.1186/1741-7015-11-21.
34. Berg RC, Nanavati J. Realist review: current practice and hereafter prospects. J Res Pract. 2016;12(one).
35. Dixon-Woods Chiliad, Sutton A, Shaw R, et al. Appraising qualitative research for inclusion in systematic reviews: a quantitative and qualitative comparison of three methods. J Health Serv Res Policy. 2007 January;12(1):42-7. doi: 10.1258/135581907779497486. PMID: 17244397.
36. Ring Due north, Ritchie 1000, Mandava L, et al. A guide to synthesising qualitative research for researchers undertaking health technology assessments and systematic reviews. University of Stirling, School of Nursing, Midwifery and Wellness. Scotland: NHS Quality Improvement Scotland; 2011.
37. Barnett-Page East, Thomas J. Methods for the synthesis of qualitative inquiry: a disquisitional review. BMC Med Res Methodol. 2009 Aug 11;9:59. doi: x.1186/1471-2288-9-59. PMID: 19671152.
38. Critical Appraisal Skills Programme. CASP qualitative checklist. [online]. Oxford: Critical Appraisal Skills Programme; 2018. https://casp-uk.cyberspace/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf. Accessed on Nov 7, 2019.
39. Sterne JA, Hernan MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016 Oct 12;355:i4919. doi: x.1136/bmj.i4919. PMID: 27733354.
40. Higgins JPT, Light-green S. Cochrane handbook for systematic reviews of interventions. The Cochrane Collaboration; 2011. www.handbook.cochrane.org. Accessed on January ten, 2017.
41. Agency for Healthcare Research and Quality. Methods guide for effectiveness and comparative effectiveness reviews. AHRQ Publication No. 10(14)-EHC063-EF. Rockville, Dr.: Agency for Healthcare Inquiry and Quality; January 2014. www.effectivehealthcare.ahrq.gov.
42. Berkman ND, Lohr KN, Ansari MT, et al. Grading the forcefulness of a body of evidence when assessing wellness care interventions: an EPC update. J Clin Epidemiol. 2015 Nov;68(eleven):1312-24. doi: x.1016/j.jclinepi.2014.11.023. PMID: 25721570.
43. Atkins D, Chang SM, Gartlehner Chiliad, et al. Assessing applicability when comparing medical interventions: AHRQ and the Effective Health Care Program. J Clin Epidemiol. 2011 November;64(11):1198-207. doi: 10.1016/j.jclinepi.2010.11.021. PMID: 21463926.
Half dozen. Definition of Terms
This section is not applicative.
7. Summary of Protocol Amendments
If we need to better this protocol, we will give the date of each amendment, describe the change and give the rationale in this section. Changes will not be incorporated into the protocol. Table 4 below illustrates the approach.
Table 4. Table of changes to protocol
| Engagement | Section | Original Protocol | Revised Protocol | Rationale |
|---|---|---|---|---|
| This should be the effective date of the change in protocol | Specify where the change would exist found in the protocol | Describe the language of the original protocol. | Describe the alter in protocol. | Justify why the change will amend the report. If necessary, describe why the change does non introduce bias. Do non use justification as "because the AE/TOO/TEP/Peer reviewer told the states to" but explain what the change hopes to accomplish. |
AE = acquaintance editor; TEP = Technical Expert Panel; As well = job society officeholder
Viii. Review of Key Questions
AHRQ posted the KQs on the AHRQ Effective Wellness Intendance Website for public annotate. The EPC refined and finalized the KQs later on reviewing public comments and obtaining input from KIs and the TEP. This input is intended to ensure that the KQs are specific and relevant.
9. Key Informants
KIs are the cease users of inquiry. They can include patients and caregivers, practicing clinicians, relevant professional and consumer organizations, purchasers of wellness care, wellness care systems, payers, and others with experience in making health intendance decisions. Within the EPC programme, the KI part is to provide advice most identifying the KQs for research that will inform wellness care decisions. The EPC solicits input from KIs when developing questions for systematic review or when identifying high-priority enquiry gaps and needed new research.
KIs are non involved in analyzing the prove or writing the report; they also have not reviewed the study, except as given the opportunity to do and so through the peer or public review mechanism.
KIs must disclose any financial conflicts of involvement greater than $v,000 and any other relevant concern or professional conflicts of interest. Considering of their function as end users, individuals are invited to serve as KIs and those who present with potential conflicts may exist retained. The AHRQ Task Order Officer (TOO) and the EPC work to residue, manage, or mitigate any potential conflicts of interest identified.
10. Technical Experts
Technical Experts constitute a multidisciplinary group of clinical, content, and methodological experts who provide input in defining populations, interventions, comparisons, or outcomes and identify studies or databases to search. They are selected to provide wide expertise and perspectives specific to the topic under evolution. Divergent and alien opinions are common and perceived as healthy scientific discourse that results in a thoughtful, relevant systematic review. Therefore, study questions, design, and methodological approaches do not necessarily represent the views of private technical and content experts. Technical Experts provide information to the EPC to identify literature search strategies and propose approaches to specific issues as requested by the EPC. Technical Experts do not practice analysis of whatever kind nor practice they contribute to the writing of the report. They have not reviewed the report, except equally given the opportunity to do so through the peer or public review mechanism.
Technical Experts must disclose any financial conflicts of interest greater than $v,000 and any other relevant business or professional conflicts of involvement. Because of their unique clinical or content expertise, individuals are invited to serve every bit Technical Experts and those who present with potential conflicts may be retained. The AHRQ TOO and the EPC work to balance, manage, or mitigate any potential conflicts of interest identified.
XI. Peer Reviewers
Peer Reviewers are invited to provide written comments on the draft report based on their clinical, content, or methodological expertise. The EPC considers all peer review comments on the draft study in preparing the last written report. Peer Reviewers practise not participate in writing or editing the final study or other products. The final study does not necessarily represent the views of individual reviewers. The EPC will complete a disposition of all peer review comments. The disposition of comments for systematic reviews and technical briefs will be published 3 months after the publication of the show study.
Potential Peer Reviewers must disclose any fiscal conflicts of interest greater than $five,000 and whatsoever other relevant business or professional conflicts of interest. Invited Peer Reviewers may non take any financial conflict of interest greater than $5,000. Peer Reviewers who disclose potential business or professional person conflicts of interest may submit comments on typhoon reports through the public comment mechanism.
XII. EPC Team Disclosures
EPC cadre team members must disclose any financial conflicts of interest greater than $ane,000 and any other relevant business or professional person conflicts of interest. Related financial conflicts of interest that cumulatively total greater than $1,000 will usually disqualify EPC cadre team investigators.
Xiii. Function of the Funder
This project was funded under Contract No. HHSA290201500011I from AHRQ, U.South. Section of Health and Man Services. The AHRQ Also reviewed contract deliverables for adherence to contract requirements and quality. The authors of this report are responsible for its content. Statements in the report should non exist construed as endorsement by AHRQ or the U.S. Department of Health and Homo Services.
XIV. Registration
This protocol will exist registered in the international prospective register of systematic reviews (PROSPERO).
Appendix A
| Search | Query | Establish |
|---|---|---|
| #one | Search ((("high utilizer" OR "high utilizers of health intendance" OR "high utilizing" OR "super utilizers" OR "super utilizing" OR "frequent utilization" OR "frequent utilisation" OR "frequent utilizers" OR "heavy utilization" OR "heavy utilizers" OR "loftier attenders" OR "echo users" OR "hyperusers" OR "revolving door patients" OR "hyperutilization" OR "overutilization" OR "recividism")) OR "frequent users") OR "frequent user" OR "medically complex" OR "loftier need" Sort past: All-time Lucifer | 3460 |
| #two | Search ((("Multiple Chronic Conditions"[Mesh]) OR "Comorbidity"[Mesh]) OR "multimorbidity" [MeSH] Sort past: All-time Friction match | 100740 |
| #iii | Search ((((((((((((((((((("Diabetes Mellitus"[Mesh]) OR "Middle Failure"[Mesh]) OR "Cardiovascular Diseases"[Mesh]) OR "Hypertension"[Mesh]) OR "Pulmonary Disease, Chronic Obstructive"[Mesh]) OR "Asthma"[Mesh]) OR "Chronic Pain"[Mesh]) OR "Headache"[Mesh]) OR "Anterior Wall Myocardial Infarction"[Mesh]) OR "Kidney Failure, Chronic"[Mesh]) OR "Dementia"[Mesh]) OR "Alzheimer Affliction"[Mesh]) OR "Lung Diseases, Obstructive"[Mesh]) OR "Stroke"[Mesh]) OR "Arrhythmias, Cardiac"[Mesh]))) OR "chronic gastrointestinal disorder") OR "Coronary Illness"[Mesh] Sort past: Best Match | 3003277 |
| #4 | Search (("Disabled Persons"[Mesh]) OR "Fragile Elderly"[Mesh]) OR "Mobility Limitation"[Mesh] Sort by: All-time Friction match | 75328 |
| #5 | Search (("health risk behaviors") OR ("Behavioral Symptoms"[Mesh]) OR "Substance-Related Disorders"[Mesh]) OR "Depression"[Mesh]) OR "Feet"[Mesh]) OR "Cognitive Dysfunction"[Mesh])) OR (("serious mental illness") OR "chronic toxic stress") Sort past: Best Lucifer | 654519 |
| #8 | Search ("Homeless Persons"[Mesh]) OR ((((((((("Social Determinants of Health"[Mesh]) OR "Social Isolation"[Mesh]) OR "Poverty"[Mesh]) OR "Educational Status"[Mesh]) OR "Literacy"[Mesh]) OR "Intimate Partner Violence"[Mesh]) OR "Medically Uninsured"[Mesh])) OR (((((("food insecurity") OR "housing instability") OR "unemployed") OR "physical safety") OR "customs deprivation") OR "adverse childhood experiences")) Sort by: All-time Match | 138695 |
| #nine | Search (#2 OR #iv OR #5 OR #8) Sort by: All-time Match | 918962 |
| #10 | Search (#three AND #9) Sort by: Best Friction match | 105820 |
| #eleven | Search (#3 AND #9) Sort by: All-time Match Filters: Humans | 103615 |
| #12 | Search (#iii AND #9) Sort by: Best Match Filters: Humans; Adult: xix+ years | 75716 |
| #13 | Search (#3 AND #ix) Sort past: All-time Lucifer Filters: Humans; English; Adult: 19+ years | 67531 |
| #xiv | Search (#three AND #nine) Sort by: Best Match Filters: Publication appointment from 2000/01/01; Humans; English language; Adult: 19+ years | 55068 |
| #16 | Search ((((((((((("Patient-Centered Care"[Mesh]) OR "Disease Management"[Mesh])) OR ((("health home") OR "Accountable Intendance Organizations"[Mesh]) OR "Managed Care Programs"[Mesh])) OR ("Community Health Workers"[Mesh]) OR "Example Management"[Mesh]) OR "care coordination") OR "patient intendance management")))) OR ((((((((((("hotspotting") OR "patient navigation"[MeSH Terms]) OR "care management") OR "multidisciplinary team intendance") OR "integrated behavioral wellness") OR "diversion strategies") OR "self management support") OR "health coaching") OR "transition care") OR "enhanced chief care") OR "interdisciplinary care")) OR "patient navigation")) OR ((((((((((("House Calls"[Mesh]) OR "Text Messaging"[Mesh] OR "dwelling visit")) OR "chemist's intendance management") OR "caregiver support")) OR "medicaid direction") OR "care direction") OR "medication help") OR "home care") OR "transitional care")) OR "warm handoff") OR "diversion squad") Sort by: Best Lucifer | 207066 |
| #17 | Search (#14 AND #16) Sort by: Best Lucifer | 1686 |
| #xviii | Search (#17 OR #ane) Sort by: Best Friction match | 5143 |
| #xix | Search (#17 OR #ane) Sort past: Best Match Filters: English language | 4987 |
| #20 | Search (#17 OR #ane) Sort past: All-time Lucifer Filters: English; Adult: xix+ years | 3229 |
| #21 | Search (#17 OR #1) Sort by: Best Friction match Filters: Humans; English language; Adult: 19+ years | 3229 |
| #22 | Search (#17 OR #1) Sort past: Best Match Filters: Publication date from 2000/01/01; Humans; English; Adult: 19+ years | 3009 |
bainbridgenoblat1948.blogspot.com
Source: https://effectivehealthcare.ahrq.gov/products/high-utilizers-health-care/protocol
0 Response to "What Is the Best Health Insurance for a Family of High Utilizers?"
Post a Comment